Diary entries by kiritaki with persistent shoulder pain participating in the StePS-NZ trial: a qualitative content analysis
Kia ora, nō Te Awamutu āhau, kō Paige tōku ingoa. My name is Paige Hughes and I am from Te Awamutu, however my whānau currently live in the Northern Territory of Australia. I am a 3rd year physiotherapy student at Te Whare Wānanga o Otāgo and during the summer of 2025/6, I had the pleasure of completing a Māori summer student studentship with the StePS-NZ research team.

Physiotherapy for rotator cuff related shoulder pain usually involves targeted exercises and manual therapy. It is also important to help kiritaki (client/patients) and their whānau to understand why they have pain, what they themselves can do for their pain (self-management), what to do when there is a flare-up, and when and where to seek healthcare when self-management is not enough. Such conversations are generally threaded throughout the physiotherapy consultations.
Researchers and clinicians increasingly believe that sharing of such knowledge (‘tangata whaiora education’) is critical for kiritaki recovery. A recent research study in Canada even showed that providing ‘only’ patient education achieved results that were comparable to providing exercise plus patient education.
The StePS-NZ study at the Otago School of Physiotherapy and four clinics across the country evaluated whether two initial sessions with targeted, individualised patient-therapist conversations ('patient education') can be as effective as starting immediately with ‘usual’, individualised physiotherapy (Usual Physiotherapy Group) for people with rotator cuff-related shoulder pain. At six weeks after the first session, those participants (Stepped Care Group) who had not yet recovered were offered usual physiotherapy that could also include manual therapy and specific shoulder exercises. This website was used in both groups as a basis for conversations about their shoulder pain. The outcomes of the two groups will be analysed and reported in journal articles.
Besides completing a number of questionnaires at various timepoints, participants made weekly online diary entries (using REDCap) over a 3-month period. They documented shoulder pain patterns, completion of exercises, and responses to the online resources that formed part of the intervention.
The aim of this analysis was to explore the content of participants’ diary entries relating to a specific question, ‘Do you have any other comments for this week?’.
What did we do?
The Stepped Care group included 97 kiritaki and the Usual Physiotherapy group had 101. After deleting all entries for the above question containing no comments, 799 entries from 152 participants remained, 73 (75%) participants of the Stepped Care and 79 (81%) of the Usual Physiotherapy Group. The Stepped Care Group had a median of 4 entries (range 1 to 12) per participant and the Usual Physiotherapy Group had a median of 5 entries (range 1 to 10). We analysed the entries using content analysis.
What did we find?
We developed 3 themes that described key parts of the participants’ haerenga (journey) – whanaungatanga (relationships), mōhiotanga (understanding) and pain and emotions as a kaitiaki (guardian/protector). These themes were guided by participants’ individual haerenga which were unique but also showed a recurring pattern that follows the themes.
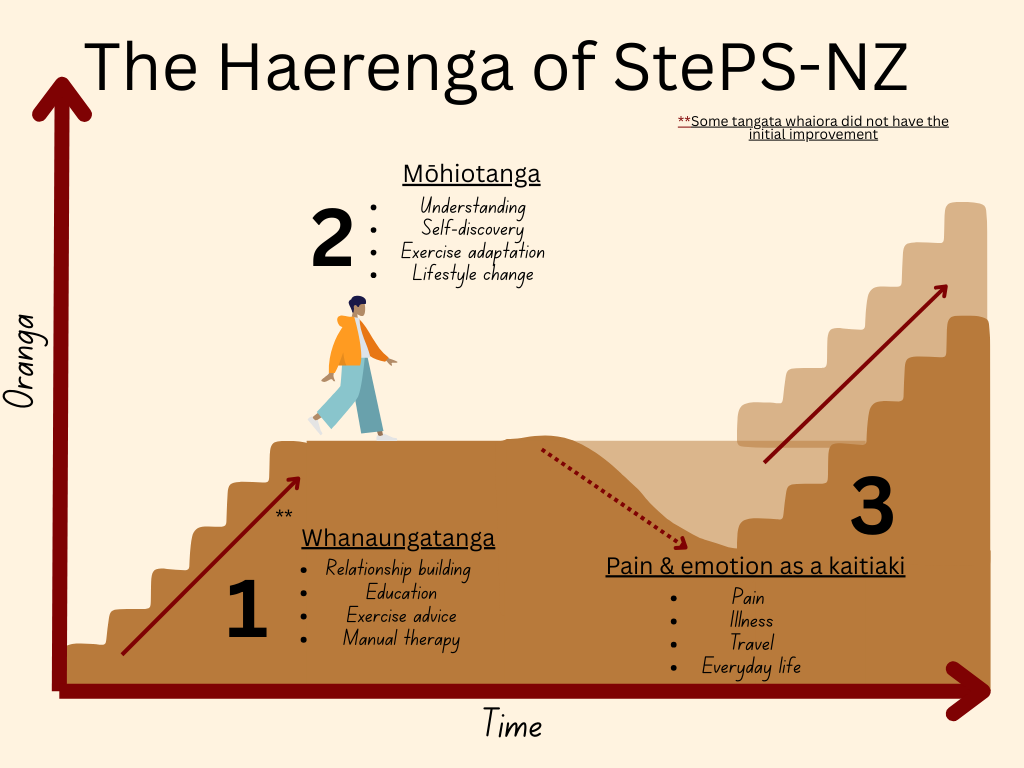
Whanaungatanga
Most participant’s haerenga initially began with whanaungatanga with clinicians, this led to an initial improvement for most participant’s oranga (livelihood, welfare). For example, one participant of the Stepped Care group expressed being “really pleased with assessment and advice” and noted “feeling confident to start building strength gradually” (#1). This comment is built upon the relationship established between clinician and participant. Whanaungatanga also relates to the participant’s relationship with their whānau and friends, providing motivation in the form of encouragement and support for some participants. These connections with the clinicians and wider whānau act as the base where the journey to rehabilitation can begin to thrive and grow.
Mōhiotanga
Education and advice played a crucial role in supporting mōhiotanga (knowledge) development for the participant and shows how this has the potential to lead to improvements. Participants with initial improvements appeared to have gained a better mōhiotanga or understanding of their presentation or condition, to find what works best for them. This was expressed as adapting exercise to suit their lifestyle, taking initiative towards physical activity to meet their own goals or even adding specific movements that they found to improve their pain or function. One participant of the Usual Physiotherapy Group shared that they were more “conscious to keep the whole shoulder moving and relaxed” as well as using “…ice packs, hot packs and daily guided medication help to provide relief” (#45).
Observations varied amongst participants, with most highlighting how movement is important for recovery. Other examples included lifestyle changes (healthy eating, reduced alcohol consumption, daily walks), self-administered massage, posture changes, exercise adaptations and an increase in general physical activity. Overall, this theme was guided by participants’ ability to adapt and themselves discover ways to alleviate pain and discomfort in a way that corresponds to their personhood. These diary entries reflected ‘listening’ to the shoulder, getting to know personal limits, and keeping symptoms under control (self-regulation).
Pain and emotion as a kaitiaki
This theme reflects the role pain and emotion had as kaitiaki (guardian) for participants. Responses varied among the participants, some experiencing increased motivation and others feeling frustration and disappointment. Some participants initially experienced increased pain or emotional responses, which decreased motivation for exercise in some cases. On the flip side, these pain experiences also acted as a guide for some participants, motivating them to continue with their chosen physical activity (examples such as walking, exercise classes or swimming). Either way, pain and emotion were protectors of the participants’ tinana (physical body), guiding them towards enhancing and/or challenging motivation.
Some participants wrote about how the new understanding about their pain helped to continue with exercises and activity: “learning that pain when starting an activity may subside when the movement is repeated was a gamechanger… I now know that low level pain is not damaging to my shoulder…” (#97, Usual Care Group). These responses were reflected in many comments and acted as a kaitiaki for participants’ self-discovery and recovery plan.
What does this mean?
It is important that clinicians recognise the uniqueness of the haerenga of each individual kiritaki, and really and truly explore that with them. Sharing of health information should be personalised to them as a person, and not just as an injury. The kiritaki should feel supported and confident to self-explore their pain patterns and manage flare-ups, yet also know when and where to seek consultations with healthcare providers.
My analysis showed diversity amongst participants’ comments across both groups of the trial. It is important that clinicians listen to their patient’s reasons for seeking care, their knowledge and beliefs about their pain and injury, also create space for them to ask questions, and to support them to explore their pain patterns and what they would like to gain from the healthcare.
Thereby, the clinician supports the kiritaki to create a platform to navigate recovery within their circle of control.
References